
The Chief Health Officer in 2026: From Medical Leader to Enterprise Risk Architect
Four Key Takeaways
- The Chief Health Officer role is shifting from clinical leadership to enterprise risk architecture, with health now viewed as a core driver of continuity, defensibility, and enterprise value.
- In 2026, boards expect CHOs to own five risk domains: workforce risk, cyber-bio risk, regulatory exposure, ESG liability, and reputational risk, with clear decision rights and escalation paths.
- Effective CHOs strengthen board governance by delivering prioritized, decision-ready health risk insights aligned to existing risk reporting structures and committee oversight.
- Board-ready CHOs combine risk architecture mindset, health data security fluency, vendor governance discipline, and board-grade communication, operating as true C-suite leaders rather than clinical administrators.
The Chief Health Officer role has reached a point of strategic reckoning. In 2026, boards are no longer asking whether their organization has a health strategy. They are asking whether their C-suite healthcare leadership can contain the risk that health-related events now represent to the entire enterprise.
This is not a clinical question. It is a governance one.
Health risk now registers in the boardroom alongside cybersecurity and regulatory exposure: as a source of operational disruption, financial volatility, and reputational consequence. The McKinsey Health Institute’s January 2026 report identified up to $11.7 trillion in potential annual global economic value tied to workforce health, and noted that many employers continue to struggle with effective action on this front.
Gartner’s 2026 research reinforces the point, explicitly positioning workforce resilience and psychological safety as core organizational responsibilities rather than peripheral HR functions.
The Chief Health Officer role is no longer most valuable as a medical advisor or benefits steward. It is most valuable as an enterprise risk architect who reduces surprise, clarifies ownership, and builds defensible decision frameworks before disruption arrives.
This blog defines what that means in boardroom terms. What risks the CHO should own, how boards should oversee them, and what makes a CHO genuinely board ready.
Why Boards Are Primed for This Now
The boardroom’s sensitivity to health-related enterprise risk did not begin in 2026. It was conditioned by the COVID-19 pandemic, and that conditioning has not faded. What boards absorbed was not a public health lesson. It was a lesson in continuity failure, workforce unavailability, and the cost of operating without defensible protocols. That memory now shapes how boards scrutinize C-suite healthcare leadership.
Human capital oversight has since moved firmly into governance territory. Deloitte’s 2025 Global Human Capital Trends report confirms that leaders who actively balance business and human outcomes are better positioned to build sustainable enterprise advantage, and that inaction on workforce risk carries greater long-term cost than intervention.
Risk reporting expectations have sharpened in parallel. McKinsey’s 2025 Global GRC Benchmarking Survey found that many boards still lack sufficient engagement in risk oversight, and that significant gaps remain between established governance frameworks and their practical execution at the C-suite level. Boards today are seeking prioritized, decision-ready risk intelligence, not long inventories of exposure with no clear ownership attached.
If health is now a recurring enterprise exposure, the Chief Health Officer must operate with the authority, fluency, and accountability of a risk leader, not a program manager.
The CHO’s Enterprise Risk Portfolio
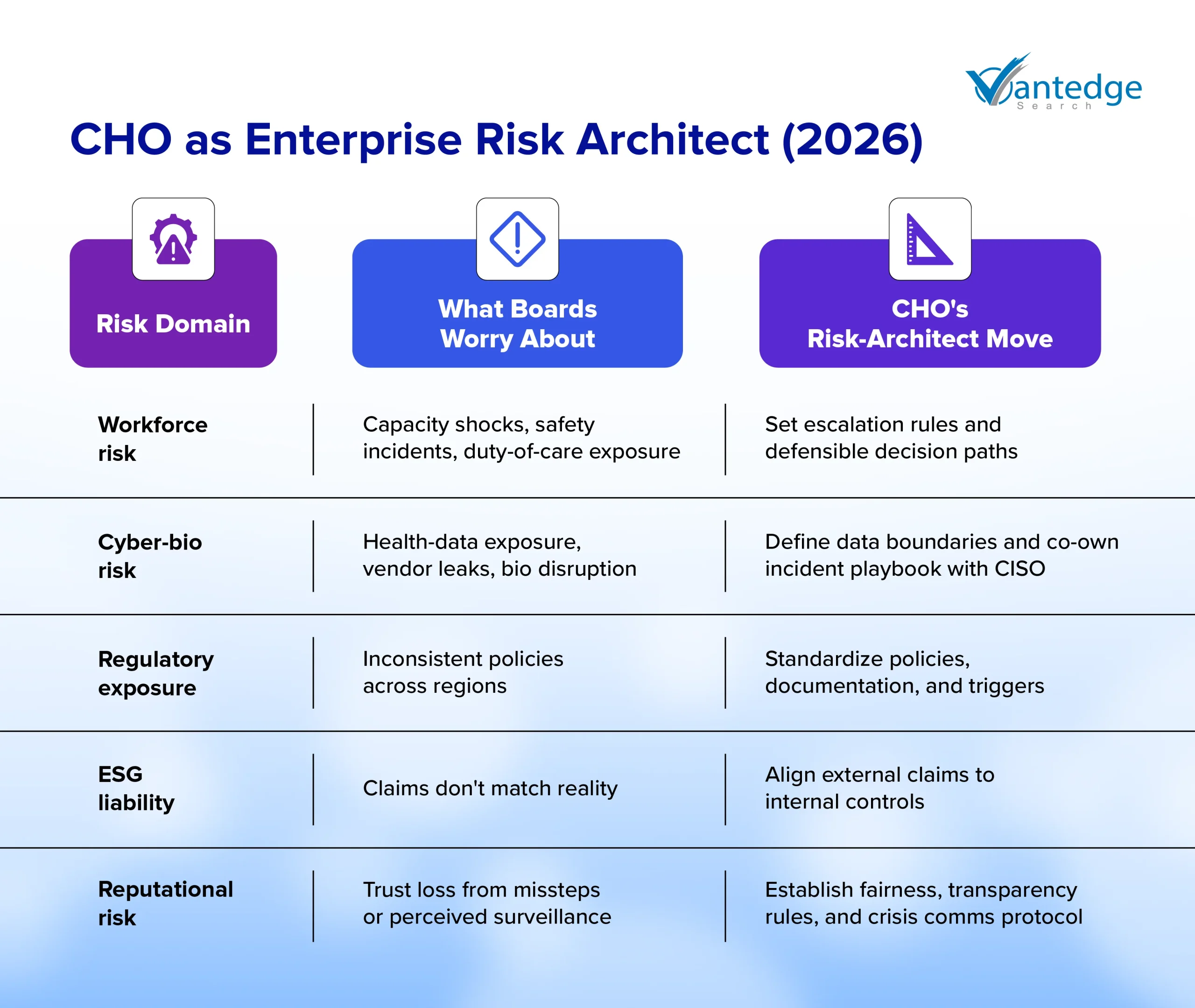
The Chief Health Officer role carries more enterprise risk surface area than most organizations formally recognize. The five domains below represent the core risk architecture responsibility the CHO must own in 2026.
Each carries distinct board exposure, a defined CHO response, and a failure mode that no organization can afford to discover reactively.
1. Workforce Risk
What it is: Workforce fragility that surfaces as capacity gaps, burnout-driven turnover, safety incidents, and performance volatility across the organization.
The McKinsey Health Institute’s January 2026 report reinforces that employee health ties directly to productivity and execution capacity, not as a wellness benefit, but as a measurable performance variable. Organizations that treat mental health and safety as programs rather than controlled exposures consistently underestimate the governance liability they are carrying.
What boards worry about: “Are we exposed on duty-of-care and safety decisions, and can we defend them consistently?”
What the CHO architects: Decision governance for high-risk workforce situations, including escalation paths, manager protocols, and documentation discipline. Workforce-risk signals are tied to execution metrics, not to program participation rates.
Failure mode: Treating mental health and safety as programs rather than controlled enterprise exposure, leaving the organization unable to defend its decisions when scrutiny arrives.
2. Cyber-bio Risk
What it is: Sensitive health-adjacent data exposure through vendors and systems, alongside biosecurity disruption risk in sectors such as life sciences, manufacturing, and travel.
Deloitte’s 2025 Life Sciences and Health Care CISO Survey found that third-party risk and health data security governance remain among the top challenges for senior cybersecurity leaders, with many organizations struggling to maintain continuous vendor monitoring at scale.
The CHO carries equal ownership of what health-related data gets collected, retained, and disclosed alongside the CIO and CISO.
What boards worry about: “What happens if health-related data is exposed, or if bio-related disruption hits operations?”
What the CHO architects: Clear boundaries on health-related data use, vendor access discipline, and a defined incident-response role that covers who speaks, who decides, what gets disclosed, and what remains off-limits.
Failure mode: Vendor sprawl and unclear ownership, where security owns systems, HR owns vendors, and no function owns end-to-end risk.
3. Regulatory Exposure
What it is: Overlapping obligations across workplace safety, accommodations, leave, privacy, and sector-specific rules that generate inconsistency risk across regions and business units.
BCG’s healthcare risk management research confirms that regulatory complexity is intensifying, and that organizations require integrated compliance frameworks rather than fragmented ownership across functions to maintain defensibility under scrutiny.
What boards worry about: “Are we consistent across regions and business units, and do we have defensible processes?”
What the CHO architects: Policy coherence across HR, Legal, and Operations; escalation and documentation standards that hold under regulatory inquiry; and scenario readiness before a crisis tests the gaps.
Failure mode: Fragmented compliance ownership that becomes reactive and creates legal exposure before leadership identifies the pattern.
4. ESG Liability
What it is: Human sustainability narratives and “S” claims becoming credibility risks when external positioning and internal governance controls do not correspond.
Deloitte’s 2025 Global Human Capital Trends research positions workforce health as a system-level governance responsibility, not a perks-based exercise. Organizations that overstate wellbeing commitments without corresponding governance structures are actively building measurable ESG liability.
What boards worry about: “Are we exposed to claims of performative or inconsistent workforce health and safety practices?”
What the CHO architects: Alignment between external commitments and internal controls; evidence discipline in what the organization publicly claims; governance that prevents overstatement before it becomes a legal or reputational event.
Failure mode: Public positioning that outruns governance, converting ESG commitment into reputational and legal exposure.
5. Reputational Risk
What it is: Trust shocks from perceived surveillance, inequitable benefit decisions, mishandled incidents, or inconsistent policy enforcement that reach employees, media, or regulators simultaneously.
BCG’s operational resilience research reinforces that organizations require clearly defined decision rights and pre-built response playbooks to prevent reputational downside from case-by-case, in-the-moment choices.
What boards worry about: “Will the company look careless or unfair under pressure?”
What the CHO architects: Principles for defensible boundaries, fairness, and transparent intent, supported by a cross-functional protocol with Legal and Communications that activates before incidents escalate.
Failure mode: Case-by-case decision-making that produces inconsistency, leaves no defensible record, and invites stakeholder backlash at the worst possible moment.
Board Governance: Reporting, Oversight, and Committee Placement
Governance without accountability architecture is exposure waiting to surface. For health risk to be managed with the same rigor as financial or cyber risk, boards need a consistent cadence, clear ownership, and reporting that drives decisions, not documentation.
What Boards Should Ask For
Effective board oversight of health-related enterprise risk does not require technical fluency. It requires the right questions, asked consistently. The reporting the CHO brings to the board should be prioritized and decision-ready, covering:
- Top health-related enterprise risks, ranked by consequence, not volume
- Clear ownership and escalation triggers for each domain
- Cross-functional dependencies across HR, Legal, CIO/CISO, and COO
- Controls in place and where gaps remain
Where Oversight Should Live
The question of committee placement matters less than the question of consistent accountability. Deloitte’s 2025 Audit Committee Practices Report confirms that ERM oversight is distributed across audit committees, full boards, and risk committees depending on organizational structure and industry, and that what differentiates effective governance is not placement but clarity of charter and cadence.
For most organizations, health risk governance sits most naturally within the risk or people/compensation committee. What the board must avoid is diffused accountability, where no single committee owns the risk and oversight becomes ceremonial.
Reporting Discipline
McKinsey’s 2025 GRC Benchmarking research confirms that the most effective risk functions communicate with boards through prioritized risk framing tied directly to strategic decisions, rather than through comprehensive inventories that require boards to self-navigate to the point.
The CHO’s reporting must meet that same standard: fewer risks, clearly owned, with defined decision implications.
Bring sharper focus to executive hiring with Vantedge Search
Executive Search Lens: What Makes a CHO Board-ready
Identifying a Chief Health Officer who can operate at enterprise scale requires a fundamentally different evaluation framework than the one used to assess clinical leadership. The question is not whether a candidate has medical credentials.
The question is whether they have the governance instincts, cross-functional authority, and risk communication discipline that board-level accountability demands.
Board-ready Backgrounds
Board-ready CHOs are not defined by a single credential or career path. They are defined by demonstrated behavior across governance situations.
Three viable archetypes that meet that standard in the Chief Health Officer role are:
- The Clinician-Executive: A medical background paired with enterprise governance exposure, cross-functional accountability, and a track record of operating above clinical program delivery.
- The Risk and Operations Leader: Deep duty-of-care and workforce safety discipline, with experience building escalation frameworks and defensible decision records.
- The Data Governance Leader: Strong privacy instincts, vendor governance maturity, and fluency in health data security at an enterprise level.
Each archetype brings a distinct entry point into risk architecture. What matters is whether the candidate has operated where decisions carry legal, financial, and reputational consequences simultaneously.
Should the CHO Sit on the Risk Committee
If the CHO owns enterprise health risk architecture rather than program delivery, a formal interface with the risk or people committee is justified. Deloitte’s 2025 survey found that nearly three-quarters of boards are spending more time on strategy development and scenario planning with senior leaders, and that C-suite representation in risk governance is becoming a baseline expectation, not an exception.
The CHO need not hold a permanent board seat to fulfill this function. A standing presenter role, tied to a defined reporting cadence and clear risk ownership mandate, is often sufficient and structurally cleaner.
Competencies That Separate Strategic CHOs from Clinical Administrators
The distinction between a strategic Chief Health Officer and a clinical administrator is not a matter of seniority. It is a matter of operating model. Forbes identifies that as people risk grows in boardroom relevance, senior HR and health leaders are expected to connect workforce decisions directly to financial and strategic outcomes, rather than advocate for programs in isolation.
The competencies that signal board-readiness in a CHO candidate are:
- Risk architecture mindset: The ability to set thresholds, define decision rights, and pre-build playbooks before incidents occur.
- Defensible data boundaries: Clarity on what health-related data the organization should and should not collect, retain, or disclose.
- Vendor governance discipline: Structured oversight of third-party health-data access with defined accountability.
- Board-grade communication: The ability to present prioritized risk intelligence that drives decisions, not detailed program inventories.
Three interview prompts that surface these qualities quickly:
- “What would you refuse to measure, and why?” This tests risk architecture judgment over compliance instinct.
- “How would you govern health-data exposure alongside the CISO?” This tests cross-functional ownership clarity.
- “How would you set escalation triggers and pre-approved responses?” This tests whether the candidate builds governance before pressure arrives.
These questions quickly reveal whether a candidate thinks like an enterprise risk architect or a clinical program owner.
Building this governance capability requires more than the right frameworks. It requires leaders who are equipped to sustain high-stakes decision-making over time. (For a grounded perspective on why leadership health matters, read our blog: Mental Health and Leadership: Supporting Wellness at the Top.)
Closing: The Standard Has Shifted
In 2026, the Chief Health Officer role becomes a genuine governance asset when the organization can make health-related decisions that are predictable, defensible, and trusted, including under pressure.
That standard does not come from better wellness programs or broader benefit coverage. It comes from risk architecture: defined ownership, documented thresholds, clear escalation paths, and cross-functional accountability that holds when regulators, boards, or the public apply scrutiny.
For boards, the signal to look for is simple. If the Chief Health Officer cannot explain boundaries, ownership, and escalation in plain language, the enterprise will keep discovering health risk through disruption, not governance.
The role is ready for board-level accountability. The question is whether the organization is ready to grant it.
If your board is rethinking the C-suite role as a business-critical leadership hire, partner with Vantedge Search today for a more disciplined search process.
FAQs
The CHO oversees workforce health strategy, manages health-related enterprise risks, and ensures the organization maintains defensible, governance-backed health decisions.
In 2026, the CHO is shifting from a clinical advisor to an enterprise risk architect, owning workforce, regulatory, ESG, and reputational risk at board level.
The CHO brings prioritized health risk intelligence to the board, defines escalation protocols, and ensures health-related decisions meet governance standards consistently.
Board-grade communication, risk architecture mindset, health data security fluency, vendor governance discipline, and cross-functional influence define an effective CHO.
Workforce health risk drives capacity gaps, turnover, safety liabilities, and performance volatility, directly affecting execution, continuity, and enterprise value.
Leave a Reply